Economic analysis part 3: Key elements of economic analysis in health
Posted on 22nd December 2021 by Ana María Rojas Gómez

This is the third in a three-part blog which will look at a few aspects of the topic in more detail like the cost-effectiveness plane, discount rates, and other key elements in health economic evaluation. Part one was an introduction to economic analysis and part two provided explanations and examples of the most common techniques in economic evaluation.
Key elements of economic analysis in health
Considering the different ways in which costs and outcomes may be determined, all analyses should make clear their methodology in relevant aspects such as as choice of perspective, time horizon, and comparator, whatever the health economic analysis.
Some basic key elements are shown and described briefly below. These elements should be considered by policymakers and researchers who conduct economic analyses.
Perspective
This is the viewpoint assumed for the analysis of costs and outcomes. It may come from the following health actors (figure 1):
-
- One or a group of patients
- Health institution
- Society
- Third-party payer
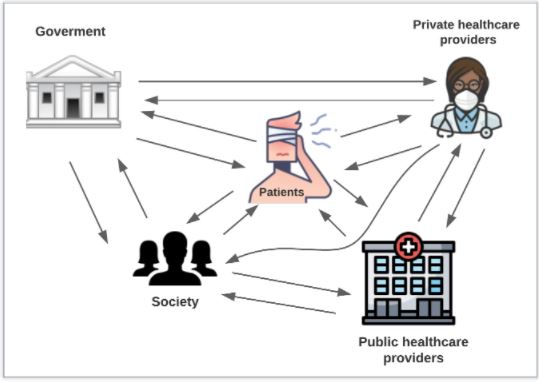
Figure 1. Health actors to consider in the perspective
Time horizon
Time in which to interpret the analysis. In this timeframe, the benefits and costs can potentially change. and should be broad enough to include, for instance, a patient’s expected lifetime (1).
Clinical effectiveness
Analysis of the additional benefit in safety, effectiveness and other outcomes should be based on a systematic review of comparative studies, RCTs primarily; nevertheless, results from experimental studies sometimes differ from real-world data. Economic evaluations should mainly use high level of evidence data, although should be used to appropriate clinical data for base cases (2).
Discount rates
This allows us to reflect on the effect of time between the costs and outcomes when the time horizon is extended for more than a year. Discounts can be on actual values. The National Institute for Health and Care Excellence (NICE) recommends the use of discount rates of 3.5% (3). However, it’s also possible to use discount rates of 0 %, 5%, 7 %, and 12 % (4). To calculate a discount rate the following formula should be used (figure 2) :
http://imgfz.com/i/yWHiTfh.png
Figure 2. Discount rate formula (5)
X = Cost or outcome of interest
r = Discount rate
t = Number of years into the future X occurs
Consider, for example, a disease diagnostic promotion campaign (Figure 3). The campaign cost $800 to implement in 2019. In addition, there is a constant increase valued at $200 per year which is produced by the number of people presenting for diagnostic.
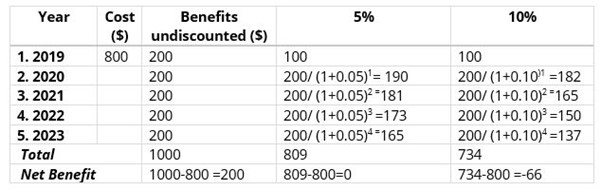
Figure 3. Hypothetical disease diagnostic promotion campaign
Given the results obtained from this exercise, this program would offer a net benefit to society.
The cost-effectiveness plane
The cost-effectiveness plane (figure 4) is used to describe the comparison between costs and health outcomes between a new and standard intervention. Four quadrants represent all combinations of possible outcomes.
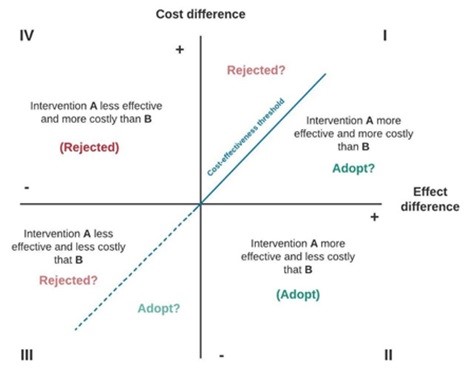
Figure 4. Cost-effectiveness plane
Intervention A is the program of interest and intervention B is the current program (status quo). So, the decision depends on which quadrant intervention A is:
- If A is in quadrant I: the choice depends on willingness-to-pay as regards the benefits of therapy.
- If A is in quadrant II: Intervention A is dominant and can be adopted.
- If A is in quadrant III: the choice depends on willingness-to-pay as regards the benefits of therapy.
- If A is in quadrant IV: intervention A is dominated and must be rejected because it is more costly and less effective.
Furthermore, the blue line indicates the cost-effectiveness threshold. This threshold often represents the maximum cost per life-year gained on which they are willing to pay for a new health technology (14).
Conclusions
Public health authorities and clinicians can use health economic evaluation to identify, measure, value, and compare the consequences and costs of the interventions being considered. These analyses support decision-making for appropriate resource allocation and maximizing benefit for the patient when resources are limited.