Expertise-based Randomized Controlled Trials
Posted on 28th February 2022 by Vinay Jaikumar

What are Expertise-based Randomized Controlled Trials ?
Conventional randomized controlled trials (cRCTs) are widely recognized as the most robust study design to evaluate a pharmacological intervention’s efficacy and safety. Their utility and internal validity is halted however when it comes to assessing non-pharmacological or surgical interventions.
Let us extrapolate the process of conventional randomization in pharmacological RCTs, where clinicians administer both interventions, to surgical RCTs. In this process, participants can be randomized to surgeons who would demonstrate preferential proficiency and expertise towards one surgical intervention over the other on grounds of familiarity, known efficiency, surgical skills, or personal opinions. (1,2)
Necessitating surgeons to perform a procedure they are less familiar or comfortable with, old or newly introduced, can lead to biased and misleading outcomes towards that procedure. Comparably, necessitating surgeons to perform a procedure they are proficient with or favor to be more efficacious can similarly lead to biased results. To mitigate this obstacle, expertise-based RCTs (EbRCTs) have emerged as an alternative to cRCTs. An EbRCT randomizes participants to surgeons with expertise in intervention A or surgeons with expertise in intervention B and they perform that specific intervention only. (3-5)
Advantages of Expertise-Based Randomized Controlled Trials
1) Differential Expertise Bias
Developing expertise in surgical interventions requires training and years of ongoing experience with the procedure. This might lead to a preference among procedures for surgeons operating a specific pathology. This leads to increased utilization of the primary procedure and in addition to familiarity can prove crucial for procedural outcomes. (2,6) Restricted expertise with surgical interventions can similarly influence procedural outcomes.
Let us consider a scenario. A cRCT is comparing procedural outcomes with an established procedure A against an established procedure B within a single center. The proportion of surgeons having more expertise with procedure A is greater than those with expertise in procedure B. Thus, a greater proportion of participants randomized to procedure A will have experienced surgeons administering the procedure. On the contrary, only a smaller proportion of participants randomized to procedure B will receive an experienced treatment. This tends to demonstrate a better but skewed procedural benefit with procedure A compared to B (Figure 1). (3-5)
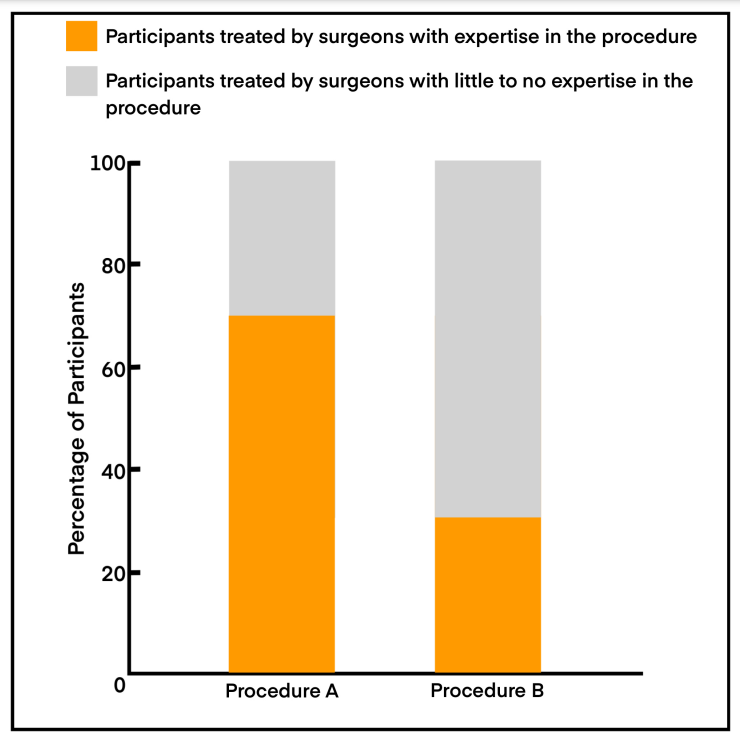
This constitutes what is called a ‘differential expertise bias.’ The greater the disproportionate expertise, the greater the differential expertise bias. Under these circumstances, an EbRCT might prove a more appropriate design to acquire accurate procedural outcomes. As participants are randomized to procedures where everyone will receive treatment from surgeons who are well versed with the procedure, both arms will demonstrate the best possible procedural outcomes, which can then be compared. (3-5)
A subset of surgical scenarios can still question the utility of EbRCT. If a cRCT compares a novel or established intervention which has a negligible technical variation to the comparator procedure, outcomes might not differ as greatly and a cRCT might just suffice. (5) The technical difficulty of a procedure can offset the benefits of expertise. Let us say a technically difficult procedure is compared against a technically effortless procedure. Even if the surgeons demonstrate equal expertise within their respective procedures (number of procedures conducted, years of experience, familiarity, or cointerventions), the technically difficult procedure might still demonstrate unfavorable outcomes, and favorable outcomes are skewed towards the less challenging procedure. (3-5)
2) Improved surgeon recruitment and reduced crossover
Under a cRCT model, surgeons can be requested to conduct procedures that deviate from their personal preference. This preference can be based on known efficacy, surgical skill, or familiarity. Surgeons might be reluctant to conduct procedures in a trial where they are necessitated to deviate from this preference. Inability to exercise this preference between two procedures in a cRCT can slow down surgeon recruitment and trial progression. However, if the procedures differ by only a minor technical variation or if the surgeon displays no preference, a cRCT design will more likely be acceptable. (3-5)
To derive accurate outcome estimates, it is pertinent that the participants receive the procedure they are randomized to. If this process were hampered, by participant crossover, the trial’s ability to determine true outcomes will be compromised. Participant crossover in surgical RCTs is facilitated, among many reasons, by surgeon bias or procedural preference. In EbRCT design, as the procedure arm is congruent with the surgeon’s preference, the tendency for participant crossover is mitigated and hence this design can offer more accurate outcomes than a cRCT. EbRCT designs have been shown to offer excellent adherence rates of participants to the respective randomized groups. (3-5)
3) Blinding and Favorable ethics
Surgeons in cRCTs are often necessarily unblinded to the procedures they perform. If surgeons are opinionated towards the efficacy or beneficence of a procedure, the tasks directed towards the trial can be subconsciously biased. The bias can manifest either as a more meticulous approach towards the preferred procedure, prescribing more efficient cointerventions, and preferentially improving procedural outcome recordings. (3-5) While EbRCT designs are not free of such bias, both procedures tend to receive the best of a surgeon’s expertise and the best of procedural outcomes.
In cRCT, we randomize participants to surgeons who perform both the intervention and control procedures. Under circumstances where surgeons do prefer one procedure over the other, we are randomizing patients to surgeons who now must perform their intervention non-preferred procedure as well. Considering the factors leading to procedural preferences, this decision will now result in substandard care and outcomes being delivered to participants which now becomes an ethical issue. An EbRCT design however randomizes patients to surgeons who only perform the procedure they are proficient in, thus eliminating the ethical concerns on delivering substandard care. (3-5)
Challenges with Expertise-Based Randomized Controlled Trials
1) Lack of Generalizability of Outcomes
If an EbRCT demonstrates a procedure to be superior compared to another, one cannot expect to obtain similar better outcomes if expert surgeons handling the inferior procedure or inexperienced surgeons handling the superior procedure start employing the superior procedure right away. Rather, both these categories of surgeons will now have to undergo a learning curve similar to that of the experienced surgeon in the EbRCT to obtain similar results with the superior procedure when they switch over. Additional factors impacting generalizability include the setting of the surgery (Explanatory/Ideal or Pragmatic/Real world) and the associated cointerventions. (3-5)
2) Logistic Constraints
EbRCT design requires surgeons practicing either of the study procedures to be situated within the same institution or hospital. In extension, the institute or hospital should house facilities for both procedures. In scenarios where this cannot be accomplished, the participant will have to be shifted to a different center which might be unacceptable to the participant in terms of additional travel or the emergency of the procedure. (3-5)
3) Sample Size
As participants are randomized to surgeons with specific expertise in a procedure, this can give rise to clustering effects. This occurs when outcome measurements from participants under a specific surgeon tend to be more alike when compared to those randomized to alternative surgeon groups. This signifies those observations are not independent and that they are correlated. This can be influenced by a surgeon’s approach to the procedure, meticulousness with the procedure, cointerventions, data recording, measurement strategies, maintaining excellent follow up, and compliance with trial guidelines. Clustering obscures true outcomes and a larger sample size will have to be recruited to derive accurate estimates. (4,5)
Conclusion
This blog summarizes the basic concepts in understanding Expertise-based Randomized Controlled Trials. Even with their inception over forty years ago, expertise-based designs remain to be utilized in only a minor subset of surgical trials. Continuing emphasis on their benefits can only improve their utility in future RCTs and enhance outcomes measurements.